Knee Ligament Repair
Ligaments are bands of tough, elastic connective tissue that surround a joint to give support and limit the joint's movement. When ligaments are damaged, the knee joint may become unstable. The ligament damage often occurs from a sports injury, road traffic accident or fall. A torn ligament severely limits knee movement, resulting in a person’s inability to pivot, turn, or twist their leg. Those individuals who cannot return to normal activities with medical treatments for a torn ligament may have the ligament repaired with surgery.
Ligaments of the knee
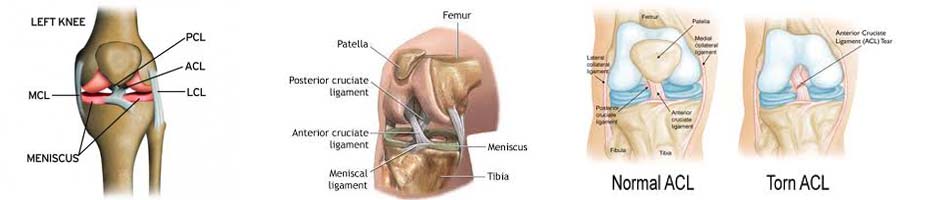
There are four major ligaments in the knee. The ligaments in the knee connect the femur (thighbone) to the tibia (shin bone):
- Anterior cruciate ligament (ACL). The ligament, located in the center of the knee, that controls rotation and forward movement of the tibia (shin bone).
- Posterior cruciate ligament (PCL). The ligament, located in the center of the knee, that controls backward movement of the tibia (shin bone).
- Medial collateral ligament (MCL). The ligament that gives stability to the inner knee.
- Lateral collateral ligament (LCL). The ligament that gives stability to the outer knee.
Reasons for the procedure
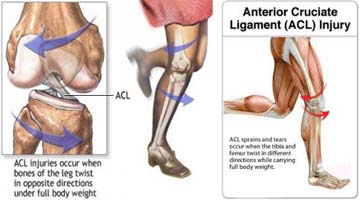
The anterior cruciate ligament (ACL) is located toward the front of the knee. It is the most common ligament to be injured. The ACL is often stretched and/or torn during a sudden twisting motion (when the feet stay planted one way, but the knees turn the other way). Skiing, basketball, and football are sports that have a higher risk of ACL injuries.
The posterior cruciate ligament (PCL) is located toward the back of the knee. It is also a common knee ligament to be injured. However, the PCL injury usually occurs with sudden, direct impact, such as in a car accident or during a football tackle.
The medial collateral ligament (MCL) is located on the inner side of the knee. It is injured more often than the lateral collateral ligament (LCL), which is on the outer side of the knee. Stretch and tear injuries to the collateral ligaments are usually caused by a blow to the outer side of the knee, such as when playing hockey or football.
Symptoms
Immediately after the injury, patients usually experience pain and swelling and the knee feels unstable. Within a few hours after a ACL injury, patients often have knee swelling, a loss of full range of motion, pain or tenderness along the joint line and discomfort while walking.
The instability caused by the torn ligament leads to a feeling of insecurity and giving way of the knee, especially when trying to change direction on the knee.
The pain and swelling from the initial injury will usually be gone after two to four weeks, but the knee may still feel unstable. The symptom of instability and the inability to trust the knee for support are what require treatment. Also important in the decision about treatment is that long-term instability leads to early arthritis of the knee.
Diagnosis
The history and physical examination are probably the most important ways to diagnose a ruptured or deficient ACL. In the acute (sudden) injury, the swelling is a good indicator.
During the physical examination ,If the ACL is torn, there will be increased forward (upward or anterior) movement of the tibia in relation to the femur and a soft, mushy endpoint when this movement ends ( Lachman’s test ).
Pivot Shift Test : In this test, if the ACL is torn, the tibia will start forward when the knee is fully straight and then will shift back into the correct position in relation to the femur when the knee is bent past 30 degrees.
X-rays of the knee are done to rule out a fracture. MRI Scan is probably the most accurate test for diagnosing a torn ACL without actually looking into the knee.

Natural History
The natural history of an ACL injury without surgical intervention varies from patient to patient and depends on the patient's activity level, degree of injury and instability symptoms.
Complete ACL ruptures have a much less favorable outcome. After a complete ACL tear, some patients are unable to participate in cutting or pivoting-type sports, while others have instability during even normal activities such as walking.
About half of ACL injuries occur in combination with damage to the meniscus, articular cartilage or other ligaments. Secondary damage may occur in patients who have repeated episodes of instability due to ACL injury. With chronic instability, up to 90 percent of patients will have meniscus damage when reassessed 10 or more years after the initial injury. Similarly, the prevalence of articular cartilage lesions increases up to 70 percent in patients who have a 10-year-old ACL deficiency.
Surgical and Non-Surgical Options
Treatment options for ACL injuries include both surgical and non surgical treatments.
Nonsurgical Treatment
Non surgical management of isolated ACL tears may be indicated in patients, who have partial or complete tears and no symptoms of knee instability during low-demand sports and who are willing to give up high-demand sports
However, people who choose not to have surgery may experience secondary injury to the knee due to repetitive instability episodes.
So, a patient who opts for non surgical treatment has to remember :
- Modification of active lifestyle to avoid high demand activities
- Muscle strengthening exercises for life
- May require knee brace
- Despite above precautions ,secondary damage to knee cartilage & meniscus leading to premature arthritis.
Surgical Intervention
ACL tears are not usually repaired using suture to sew it back together, because repaired ACLs have generally been shown to fail over time.Therefore, the torn ACL is generally replaced by a substitute graft made of tendon. The grafts commonly used to replace the ACL include :
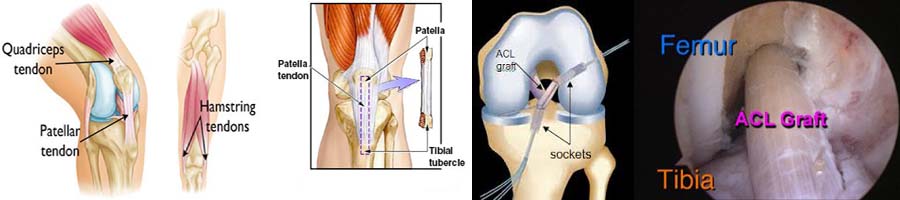
- Patellar tendon autograft
- Hamstring tendon autograft
- Quadriceps tendon autograft
Patients treated with surgical reconstruction of the ACL have long-term success rates of over 95 percent. Recurrent instability and graft failure are seen in approximately 1-2 percent of patients. The goal of the ACL reconstruction surgery is to prevent instability and restore the function of the torn ligament, creating a stable knee. This allows the patient to return to sports. There are certain factors that the patient must consider when deciding for or against ACL surgery.
Patient Considerations
Active adult patients involved in sports or jobs that require pivoting, turning or hard-cutting as well as heavy manual work are encouraged to consider surgical treatment.This even includes older patients . Activity, not age, should determine if surgical intervention should be considered.
Surgical Choices
- The middle third of the patellar tendon of the patient, along with a bone plug from the shin and the knee cap is used in thepatellar tendon autograft.
- The semitendinosus & gracilis hamstring tendons on the inner side of the knee are used in creating thehamstring tendon autograft for ACL Reconstruction. This creates a four-strand tendon graft. Hamstring graft have fewer problems associated with harvesting of the graft compared to the patellar tendon autograft including
- Fewer problems with anterior knee pain or kneecap pain after surgery
- Less postoperative stiffness problems
- Faster recovery
Postoperative Course
Physical therapy is a crucial part of successful ACL surgery, with exercises beginning immediately after the surgery. Much of the success of ACL reconstructive surgery depends on the patient's dedication to rigorous physical therapy.
In the first 10 to 14 days after surgery, the wound is kept clean and dry, and early emphasis is placed on regaining the ability to fully straighten the knee and restore quadriceps control. The knee is iced regularly to reduce swelling and pain. We use a postoperative brace or crutches to keep some or all of the patient's weight off of the surgical leg.

Rehabilitation
The goals for rehabilitation of ACL reconstruction include reducing knee swelling, maintaining mobility of the kneecap to prevent anterior knee pain problems, regaining full range of motion of the knee, as well as strengthening the quadriceps and hamstring muscles.
Neuromuscular training includes exercises to improve balance, joint control, muscle strength and power.
The patient may return to sports when there is no longer pain or swelling, when full knee range of motion has been achieved, and when muscle strength, endurance and functional use of the leg have been fully restored . This usually takes 4 to 6 months. Ideally you are able to resume all, your previous lifestyle activities including participating in sports.